News

Newswise — BOSTON –
People who suffer from insomnia are three times more likely to report thoughts of suicide and death during the past 30 days than those without the condition, reports a new meta-analysis from researchers at the Perelman School of Medicine at the University of Pennsylvania. The study is the first to control for depression and anxiety and evaluate in-depth the relationship between the broadly defined terms of insomnia and suicidality to reveal trends that may inform future targeted treatment for 32 million individuals struggling with insomnia in the United States each year. The findings (abstracts #0409 and #422) will be presented at SLEEP 2017, the 31st Annual Meeting of the Associated Professional Sleep Societies LLC (APSS).
The researchers evaluated self-report survey data assessing insomnia, depression, and anxiety symptoms among 1,160 U.S. Army servicemembers (84 percent male and average age of 31). Controlling for anxiety and depression, the researchers mapped suicidality into multiple dimensions: thoughts of killing oneself, having a plan to commit suicide, intention to kill oneself, thoughts of death (wishing you were dead), and telling people you want to commit suicide. They separated insomnia sufferers into sub-groups – those who have so-called global insomnia (insomnia as a general term), initial (trouble falling asleep at the beginning of the night), middle (trouble maintaining sleep), and terminal insomnia (waking too early from sleep), and nocturnal awakenings (frequently waking up at night) – and studied the association between each of those subgroups and dimensions of suicidality.
The team found that 2.3 percent of those in the population without insomnia reported any indices of suicidality, while 13.1 percent of those experiencing insomnia reported at least one type of suicidality. The group also found a significant association between insomnia and suicide (which echoes earlier studies), but the new research parsed out the broad concepts of insomnia and suicide to explain what aspects of these two are related in a population of military personnel.
Even after eliminating the established role of depression and anxiety in suicide, people who suffer from insomnia are three times more likely to report thoughts of suicide and death during the past 30 days. Insomnia was also found to be a significant predictor for suicidality. Although waking up multiple times throughout the night was significantly associated with greater suicidal ideation, the team was surprised that having difficulty maintaining sleep in the middle of the night was actually associated with a lower likelihood of having thoughts of suicide or having a suicidal plan. This does not mean that those at risk for suicide should try keeping themselves up during the middle of the night, however.
The association between awakenings and suicidality follows senior author Michael Perlis’ “sleep of reason” hypothesis, such that, risk for suicidality is highest as someone is awake with insomnia at night when their ability to reason, think rationally, and engage in impulse control are lowest. The team’s findings suggest that the increased awakenings at night and the decreased executive function associated with it foster dimensions of suicidality in those who are pre-disposed to thinking about committing suicide.
“It’s a bad thing to be awake when reason sleeps,” said Michael Perlis, PhD, an associate professor of Psychiatry and director of the Behavioral Sleep Medicine program, and senior author on the research. “Being awake at night, coupled with the decreased frontal lobe function that happens with sleep loss may explain the mechanism for how insomnia relates with suicide risk.”
Frequently waking up throughout the night was the only type of insomnia associated with four of the five dimensions of suicidality. One possible explanation for this finding may be that it is related to other comorbid conditions, such as obstructive sleep apnea and chronic pain.
“Middle insomnia might give them an external factor to attribute to their distress,” said Ivan Vargas, PhD, a postdoctoral fellow and first author of abstract (#0409). “Most of the participants in this study were not presently depressed - so they’re less likely to internalize stress and subsequently experience suicidal ideation. Following a night of insomnia, they may be more likely to attribute any daytime impairment to their poor sleep and not to themselves. In this case, insomnia would buffer their negative attributions about themselves and lower their risk for suicidality. This really speaks to the dynamic relationship between insomnia and depression in predicting suicidality. ”
The authors note that further research may benefit from studying this in additional populations, or in a majority female population.
Previous research from the Perlis team has shown that suicides are more likely to occur after midnight than during the daytime or evening and another study showing that more sleep reduces suicide risk in those with insomnia.
In addition to Vargas and Perlis, additional authors on (#0409) include Amy Gencarelli, from Penn, Alexandria Muench from the Philadelphia College of Osteopathic Medicine, Elaine Boland from the Cpl. Michael J. Crescenz VA Medical Center, Jennifer R. Goldschmied from Penn, and Philip Gehrman, from Penn and the Cpl. Michael J. Crescenz VA Medical Center, and additional authors on (#0422) include Amy Gencarelli, from Penn, Waliuddin Khader, from Penn, Alexandria DiGuiseppe from the Philadelphia College of Osteopathic Medicine, Jennifer Goldschmied from Penn, Elaine Boland from the Cpl. Michael J. Crescenz VA Medical Center, and Philip Gehrman from Penn and the Cpl. Michael J. Crescenz VA Medical Center.
###


Newswise —
Guidelines by the National Comprehensive Cancer Network (NCCN) recommend testing for seven known genetic changes in patients with Acute Myeloid Leukemia (AML). A study presented today at the American Society for Clinical Oncology (ASCO) Annual Meeting 2017 shows that only 67 percent of 259 evaluated patients received any genetic testing. Of the 173 patients that received any genetic testing, only 9 percent received all seven of the NCCN-recommended genetic tests.
“We now know a tremendous amount about the genetic underpinnings of the disease. We can test for these genetic changes in the clinic to see what’s making a patient’s disease tick. And often there are targeted therapies that can be matched with these genetic changes. But there’s a disconnect between what can be done, what should be done, and what is being done,” says Daniel A. Pollyea, MD, MS, investigator at the University of Colorado Cancer Center, clinical director of Leukemia Services at the CU School of Medicine, and the study’s lead author.
For example, FLT3 is a commonly mutated gene with several drugs in clinical development to specifically target this mutation. But this drug can only be used once genetic testing pinpoints the patients likely to benefit, namely those with FLT3 activation. Additional targeted treatments for AML are in development, such as Pollyea’s own work with the drugs AG-120 and AG-221, which target the 15-20 percent of AML harboring mutations in the genes IDH1 and IDH2.
Previously, the majority of data describing rates of genetic testing in AML patients have come from clinical trials, where adherence to guidelines is, as expected, very high. The current study hoped to evaluate adherence to genetic testing guidelines in AML treated outside clinical trials, in academic medical centers and in community settings. The data comes from the new, unique resource of the CONNECT MDS/AML Disease Registry, which collects treatment and outcome statistics from 86 sites distributed across the United States. Current results reflect data gathered from 2013 to 2016.
Overall, rates of patients receiving any genetic testing were higher in patients treated at academic medical centers than those treated at community clinics (76 percent versus 62 percent); higher in patients younger than 65 years old than in older patients (83 percent versus 60 percent); and higher in patients with non-Medicare insurance than in patients with Medicare (74 percent versus 61 percent).
“Basically, we’re not seeing adherence to these guidelines. It’s still a big challenge for a lot of institutions,” Pollyea says. He points out that often a major barrier to genetic testing in AML (and many other cancers) is the willingness of insurance companies to pay for testing. He also suggests that with adherence to these guidelines so low, perhaps the guidelines themselves need adjustment, though, “I think the guidelines are pretty solid and, in my opinion, I would say they don’t go far enough in recommending genetic testing,” he says.
The major accomplishment of the current study may be setting a baseline against which future data can be measured.
“We’re in our infancy with this testing, and even earlier than infancy in seeing how we’re doing on testing. But now with this registry we at least have the infrastructure available to ask these kinds of questions,” Pollyea says.
As known genetic drivers of AML are successfully paired with targeted treatments and more of both are discovered, genetic testing is likely to become an even more essential component of clinical care. Now with an understanding of the current state of genetic testing in AML, Pollyea and colleagues will be able to evaluate changes in these data as diagnostic, prognostic and treatment options evolve.

Newswise —
When teens have troubling thoughts or are prompted by a peer’s concerning behavior or news story to educate themselves on mental health, they often turn to internet search engine links – many hosted by unreliable sources.
To help combat misinformation, the Traumatic Loss Coalitions for Youth (TLC), New Jersey’s primary youth suicide prevention program at Rutgers’ University Behavioral Health Care, has launched TLC4Teens (tlc4teens.org), a resource website for children, which includes organizations, hotlines and relevant articles that have been vetted by TLC. Many also are listed on the Substance Abuse and Mental Health Services Administration’s National Registry of Evidence-based Programs and Practices.
Funded by the New Jersey Department of Children and Families, TLC4Teens links to state and national resources for issues such as grief, suicide prevention, mental health, depression, substance abuse, dating, bullying, anxiety, self-care, underage drinking, sexuality and gender identity.
A parent section includes resources on how to understand and handle a child’s grief or emotional or behavioral crises.
“The site was designed to give children easy access to the information they seek online with minimal clicks,” says Maureen Brogan, TLC statewide coordinator. “It also features a video by Olympic Gold medalist Laurie Hernandez, who reminds her fellow teens that seeking help is not a weakness and that they should use the site as a ‘resource to connect to in difficult times.’”
Brogan encourages children as young as elementary school who are using mobile devices to bookmark the site. “Children are being exposed to vicarious traumas on the internet through their smartphones or iPads. They can’t escape this and it shatters their assumptions that the world is a safe place to be – which causes stress,” she explains.
In her outreach with TLC, Brogan is seeing stressors, such as concerns over grades, that usually don’t manifest until high school occur at younger ages. While these children might not have anxiety and depression at a clinical level, the stress can become disruptive to their everyday lives, she says.
“Through education, we can empower students to watch for concerning signs among their peers or siblings and know what to do if a situation arises,” Brogan says. “We want to encourage resiliency so they can get the help they need and say ‘OK, I’ve got this.’”
Newswise —
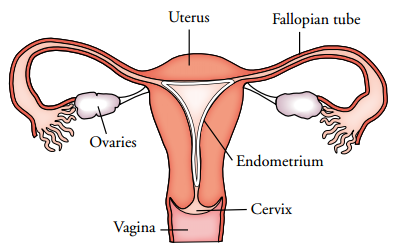
Children with differences of sex development (DSD) are born with reproductive organs that are not typically male or female. They may face infertility from abnormal development of testes or ovaries, and in some patients these organs are surgically removed to prevent an increased risk of germ cell cancer. With advancing techniques, however, children with DSD may be able to preserve their fertility for the future. This potential also presents important ethical issues, which are examined in an article published in the Journal of the Endocrine Society.
“Our earlier research suggests that in children with DSD, we might be more successful in preserving fertility at younger ages,” says senior author Courtney Finlayson, MD, from Stanley Manne Children’s Research Institute at Ann & Robert H. Lurie Children’s Hospital of Chicago. “This poses a dilemma in terms of the ideal timing for surgical removal of testes or ovaries for patients who need it. If we wait until the age of majority, when the patient can give consent, we might miss the opportunity for fertility preservation. And yet we might want to delay the surgery since we must also take into account a person’s sense of self as a man or a woman and autonomous decision making. It is a delicate balance.”
Fertility preservation techniques involve preserving at very low temperatures the mature or immature tissue from the testes or ovaries. The procedure is still experimental for pre-pubertal patients, since it relies on the development of technologies to mature germ cells in the lab. Given the uncertainty of success, there is concern that these techniques can lead to false hope for patients and parents.
Cost and insurance coverage are additional concerns. Fertility preservation is expensive, ranging from thousands to tens of thousands of dollars. It is rarely covered by insurance and is mostly considered an elective procedure.
“We can make an argument that fertility preservation in children with DSD should be covered by insurance since DSD treatment can cause infertility, which can result in serious psychological distress,” says Finlayson, an endocrinologist with the Gender and Sex Development Program at Lurie Children’s and an Assistant Professor of Pediatrics at Northwestern University Feinberg School of Medicine. “Lack of insurance coverage significantly limits access to preserving future fertility in these children.”
Because many DSD are genetic conditions that can be inherited, there is also concern about transmission to offspring. Some ethicists argue that it is irresponsible to knowingly have children with a medical condition or disability. On the other hand, advocates assert that people with disabilities can lead happy, productive lives. Furthermore, many with DSD object to their condition being referred to as a disorder or disease. In either case, adults concerned about having children with the same condition could benefit from pre-implantation genetic screening of embryos.
Another ethical consideration revolves around gender dysphoria, or the distress that some individuals with DSD experience when their early sex assignment does not match their eventual gender identity. For example, youth initially assigned male but identifying as female might feel emotional distress at providing sperm for fertility preservation. Also, high-dose estrogen or testosterone required for fertility preservation can cause irreversible physical changes that are inconsistent with gender identity.
“There are no easy answers to any of these ethical concerns,” says Finlayson. “Fertility-related care for children with DSD is in its infancy. We must carefully consider the unique ethical issues that fertility preservation presents in this population.”
Research at Ann & Robert H. Lurie Children’s Hospital of Chicago is conducted through the Stanley Manne Children’s Research Institute. The Manne Research Institute is focused on improving child health, transforming pediatric medicine and ensuring healthier futures through the relentless pursuit of knowledge. Lurie Children’s is ranked as one of the nation’s top children’s hospitals in the U.S.News & World Report. It is the pediatric training ground for Northwestern University Feinberg School of Medicine. Last year, the hospital served more than 198,000 children from 50 states and 51 countries.
SEE ORIGINAL STUDY

Newswise —
A genetic test that helps doctors determine how best to treat breast cancer—and whether chemotherapy is likely to help—is significantly more likely to be administered to white women than blacks or Hispanics, a Yale study has found.
Women of color have less access to the Oncotype Dx test, mammography and radiation treatments.
The test, called Oncotype Dx (ODx), uses gene expression to gauge how early-stage breast cancer is affecting patients’ gene activity. It uses the information to determine how likely cancer recurrence would be, and physicians and their patients can use that knowledge to decide how to proceed with treatment.
Yale researchers retrospectively analyzed a group of more than 8,000 Connecticut women who were diagnosed with hormone receptor positive breast cancer between 2011 and 2013, and found “significant racial and ethnic disparities in use of this new gene test,” said study leader Dr. Cary Gross, a member of Yale Cancer Center and professor of medicine and epidemiology at Yale School of Medicine.

Newswise — GAINESVILLE, Fla. ---
A glass of milk packs a nutritious punch, a reminder of the importance of dairy in our diets as we enter National Dairy Month, a University of Florida nutrition expert said.
“Basically, cow’s milk helps to meet nutrient needs, and some research suggests it may help to protect against some of the major chronic diseases,” said Gail Kauwell, a professor in food science and human nutrition.
Dairy food nutrients play many important roles in maintaining good health, so Kauwell encourages milk as part of a healthy eating pattern. Some key nutrients in milk include calcium, vitamins D and B12, potassium and protein. These nutrients build strong bones and teeth, maintain and improve bone mass, make red blood cells, synthesize DNA and maintain healthy blood pressure, said Kauwell, a faculty member at the UF Institute of Food and Agricultural Sciences.
For example, studies support an association between higher dairy food intake and lower risk for type 2 diabetes, said Kauwell, although she cautions that these studies do not prove cause and effect.
All sorts of “milk” fills the grocery store dairy case. So how do consumers distinguish between them? Further, what do you do if you cannot consume a certain type of dairy product?
Kauwell explained that several of the key vitamins and minerals naturally present in cow’s milk are only present in soy, almond, rice and coconut beverages if they are added to the product. And when it comes to protein, only soy beverages provide an amount equal to that of cow’s milk.
People who are lactose intolerant may be able to drink small amounts of milk without experiencing any symptoms but may prefer to drink lactose-free milk or a fortified soy beverage. On the other hand, some people cannot drink cow’s milk because of a food allergy. Those with a food allergy to milk, and those practicing a vegetarian or vegan diet also may choose to drink a fortified soy beverage, said Kaley Mialki, a UF/IFAS graduate and registered dietitian.
“If individuals are watching their weight, switching from full-fat milk, cheese and yogurt to low-fat or fat-free milk products can reduce calorie and fat consumption but still allow for intake of other important nutrients like protein, vitamins and minerals,” Mialki said.
-30-
The mission of the University of Florida Institute of Food and Agricultural Sciences is to develop knowledge relevant to agricultural, human and natural resources and to make that knowledge available to sustain and enhance the quality of human life. With more than a dozen research facilities, 67 county Extension offices, and award-winning students and faculty in the UF College of Agricultural and Life Sciences, UF/IFAS works to bring science-based solutions to the state’s agricultural and natural resources industries, and all Florida residents. Visit the UF/IFAS web site at ifas.ufl.edu and follow us on social media at @UF_IFAS.

Newswise — ST. LOUIS –
Children with complex medical conditions and those who are just in need of a regular teeth cleaning will soon have a new program devoted to their care.
Saint Louis University’s Center for Advanced Dental Education (CADE) will begin a pediatric dentistry residency program on July 1, 2017. The program, six years in the making, received initial accreditation from the Commission on Dental Accreditation in February.
SLU’s pediatric program is the only residency program of its kind in eastern Missouri or southern Illinois.
The two-year graduate program provides dentists an opportunity to study and receive clinical experience in treating children. Residents learn advanced diagnostic and surgical procedures, along with oral pathology, child-related pharmacology, radiology, child development, management of oral/facial trauma, care for patients with special needs, conscious sedation and general anesthesia.
CADE currently offers specialty training in endodontics (root canals), orthodontics (braces) and periodontics (treatment of gum disease and implants).
“We are really excited to get this program started – it will be tremendous for the region,” said John Hatton, DMD, executive director of CADE. “There are so many children in the area that have nowhere to go for their dental needs.”
Hatton said early intervention is important in dental health.
“Through CADE’s other programs, a person can have a tooth extracted instead of a root canal, not replace a missing tooth with an implant and function without braces,” Hatton said. “And now, with our new pediatric dentistry program, we can intervene early to improve a child’s oral health, which makes a difference for the rest of their life.”
SLU’s program will admit three students in its first year and another three the following year. Applicants must have a strong academic background and clinical skills, as well as a passion for working with children.
“Pediatric dentistry is more than just being child-friendly,” said Dan Stoeckel D.D.S., MS, pediatric dentistry graduate program director. “You have to enjoy working with kids and also work within the growth and development of a child’s mouth. Children can have extensive needs that are not the same as those of an adult patient.”
Residents admitted to the program will serve patients in a clinical setting at CADE and, when necessary, perform dental care under general anesthesia at SSM Health Cardinal Glennon Children’s Hospital.
“We will treat the patients of general pediatrics and the specialty clinics of SSM Health Cardinal Glennon Children’s Hospital, as well as provide a dental home for children from birth to age 12,” Stoeckel said.
SLUCare physicians at Danis Pediatric Center at SSM Health Cardinal Glennon Children’s Hospital will directly refer low-income patients to the pediatric dental clinic for regular cleanings and checkups.
“Small steps to improve oral hygiene can have a big impact on overall health,” Stoeckel said. “We will work with our patients to create a personalized preventative care plan for oral health.”
The clinic will also care for children with additional medical needs, ranging from those with blood disorders and cancer patients, to patients who have autism and Down syndrome.
“Residents will see patients with needs ranging from basic cleanings to complicated restorative dentistry,” Stoeckel said. “They also will learn how to manage patients that come into the clinic with a high level of anxiety.”
The residents also will provide on-call emergency dentistry coverage at Cardinal Glennon.
In February 2016, the Glennon Guild donated $50,000 to support the renovation and equipping of the Pediatric Dental clinic at the Center for Advanced Dental Education. The clinic opened Nov. 30.
“I think once we have the residents on board we will be able to see 5,500 patients a year, with 1,800 of those being unique visitors,” Stoeckel said.
Appointments are now being accepted for late summer at 314-977-PEDO (7336). All forms of Missouri and Illinois Medicaid are accepted.
The Center for Advanced Dental Education’s mission is to achieve the highest level of excellence in scholarship and patient care while educating dentists in the specialties of orthodontics (tooth straightening), endodontics (root canal treatment), periodontics (gum disease therapy) and pediatric dentistry. The center aims to serve its students, the profession of dentistry, the community of St. Louis, and the communities in which the graduates of CADE will practice their dental specialty.

Newswise —
Texas communities facing a rural hospital closure should not solely concentrate on whether or not to close a hospital, but instead focus on the available health resources in the surrounding area. That’s one of the findings of a new report by the Texas A&M Rural and Community Health Institute (RCHI) that examined rural hospital closures and looks at new solutions for rural healthcare concerns. The Episcopal Health Foundation (EHF) sponsored the report.
The report found that options like expanding telemedicine, converting a former hospital into a freestanding emergency room, or establishing new rural health clinics are some of the many successful healthcare alternatives available to communities at risk of losing a traditional rural hospital.
See the complete report: http://bit.ly/2qB7cpp
“We still have an American concept that every town should have a hospital,” said Nancy Dickey, MD, RCHI’s executive director, president emeritus of the Texas A&M Health Science Center and co-author of the report. “But the growing reality is that it’s not cost effective. The good news is there’s a menu of alternatives that can help optimize healthcare for a rural community, not shut down healthcare in that community.”
More than 3 million Texans live in rural areas and the report clearly shows the growing health crisis they face. Rural Texans are more likely to be uninsured, have lower incomes, and higher rates of death from heart disease and stroke.
Researchers found the health gap between urban and rural areas is widening and the number of physicians working in rural areas continues to fall. They point to statistics showing that 158 counties in Texas (with a combined population of 1.9 million) do not have a general surgeon and 147 counties (1.8 million people) don’t have an obstetrician/gynecologist. In 35 Texas counties, there is no physician at all.
The report also found that since 2010, more than 15 percent of the rural hospitals that have closed across the U.S. are in Texas.
“Policy makers, elected officials and communities themselves need to better understand the health challenges facing rural areas,” said Elena Marks, EHF’s president and CEO. “This report shows that the question to ask isn’t only whether to close or not close a rural hospital. It stresses the importance of regional partnerships and collaborations that can help develop a system of accessible health services that meet the unique needs of each community.”
In the report, researchers examined rural hospital closures across the country and interviewed former leaders of shuttered hospitals. While the report found that most rural hospitals in Texas closed due to financial difficulties and lack of patient volume, it also found that there are often available healthcare delivery resources within a radius of 20 to 30 miles from the closed facility.
“It’s not about miles, it’s about minutes,” Dickey said. “We need to have a policy discussion at the state and national level to determine what is an acceptable timeframe to reach care. Geography confirms that every community is a little different.”
Researchers suggest communities facing a hospital closure first ask community members where they currently go for healthcare services. Then, leaders can use that information to create a tool to help at-risk hospitals search for alternatives and develop area partnerships that create an inventory of resources without duplicating care.
“There are opportunities for these communities to reframe the health conversation and go beyond ‘Why are they closing my hospital?’” Dickey said. “There are a variety of solutions and if large hospital systems and rural hospitals can work together, they can find patient-centered answers for at-risk communities.”
About Texas A&M Health Science Center Texas A&M Health Science Center is Transforming Health through innovative research, education and service in dentistry, medicine, nursing, pharmacy, public health and medical sciences. As an independent state agency and academic unit of Texas A&M University, the health science center serves the state through campuses in Bryan-College Station, Dallas, Temple, Houston, Round Rock, Kingsville, Corpus Christi and McAllen. Learn more at https://vitalrecord.tamhsc.edu/ or follow @TAMHSC on Twitter.
Newswise —
Researchers at Johns Hopkins Medicine report new evidence that immune cells infected with a latent form of human immunodeficiency virus (HIV) are able to proliferate, replenishing the reservoir of virus that is resistant to antiretroviral drug therapy. Although HIV can be controlled with therapy in most cases, the proliferation of such reservoir cells pose a persistent barrier to developing a cure for HIV, researchers say.
“We knew before that the reservoir is very long lived,” says Robert Siliciano, M.D., Ph.D., professor of medicine at the Johns Hopkins University School of Medicine, “but what we didn’t know was how the reservoir was maintained. Now it is clear that these cells aren’t just sitting there but are dividing and replenishing themselves.”
A report on the new research, published March 24 in the Journal of Experimental Medicine, says resting CD4+ T cells not only make up the latent reservoir of HIV in those infected, but also have the potential to reactivate the production of active virus throughout the body.
In the study, Siliciano and his team collected latently infected HIV cells from the blood of 12 patients with HIV on long-term antiretroviral therapy.
After growing the CD4+ T cells in the laboratory, the investigators exposed them to four rounds of chemicals designed to stimulate cell division and proliferation.
After each round of stimulation, the cell population was split into two separate groups and allowed to grow, one serving as a control and the other used to repeat the process. Following each stimulation, the researchers also measured whether the cells were releasing HIV.
Previously, Siliciano explains, researchers suspected that such cells could not proliferate without releasing the active form of HIV. Although some cells did release HIV during the first stimulation, the subsequent stimulations of each cell line also released more virus, suggesting that some of the latently infected cells divided without releasing the infectious virus and maintained the ability to do so in subsequent stimulations.
The researchers then sequenced the genomes of the viruses. They speculated that if the viruses in subsequent stimulations from each patient were genetically identical, that would tell them the HIV they detected originated from cell division, rather than from independent infections because of HIV’s high genetic mutation rate.
“When you sequence HIV from a patient, you typically get a huge variety of HIV viruses that are genetically different. Looking at the viruses we grew out, there was much less diversity. In fact, the sequences were mostly identical throughout the series of stimulations. We think that strongly suggests that what we are seeing is a single cell proliferating and copying the HIV DNA along with it,” Siliciano says.
Siliciano’s team found that these kinds of viral copies were so common they could find multiple cells carrying the same variant of HIV in a single blood sample. “For this to be possible, the reservoir must be mostly composed of these cellular clones.”
In the future, Siliciano and his team say they will search for specific factors that cause these cells to proliferate and to develop new techniques that allow them to study whether the location of the HIV genome in the cell’s DNA affects this process.
More than 1.2 million people in the U.S. are living with HIV and one in eight of them are unaware that they are infected, according to the Centers for Disease Control and Prevention. Stigma and discrimination around HIV is still a major challenge to reaching and treating infected people, so the CDC estimates that only half of infected people have their virus under control with consistent treatment. However, the number of new HIV cases has fallen significantly since the 1990s and with improved awareness and improved treatments, the life expectancy of people infected with HIV is close to that of the general population. “Treatments now are so good,” Siliciano says, “that if we are able to eliminate the reservoir, we could cure HIV.”
Other researchers involved in this study include Nina Hosmane, Kyungyoon Kwon, Katherine Bruner, Adam Capoferri, Subul Beg, Ya-Chi Ho and Janet Siliciano of the Johns Hopkins University School of Medicine, Daniel Rosenbloom of the Columbia University Medical Center and Brandon Keele of the Fredrick National Laboratory for Cancer Research.
This work was supported by the National Institute of Allergy and Infectious Diseases Extramural Activities Martin Delaney CARE and DARE Collaboratories (AI096113 and 1UI9AI096109), an ARCHE Collaborative Research Grant from the Foundation for AIDS Research (amfAR 108165-50-RGRL), The Johns Hopkins Center for AIDS Research (P30AI094189), the National Institutes of Health (43222), the Howard Hughes Medical Institute, the Bill and Melinda Gates Foundation, and the National Cancer Institute and National Institutes of Health (HHSN261200800001E).

Newswise —
With a number of high-profile cases of prescription medication prices suddenly skyrocketing, people naturally start to wonder if perhaps some government control over the price of drugs might be a good idea. However, due to the high risk and high cost of developing new drugs, it’s possible that capping the amount of money that can be made from them would suppress development of new therapeutics.
“If we have price controls, on the one hand, it seems like a good thing for the consumer,” said Mansoor A. Khan, RPh, PhD, professor and vice dean of the Texas A&M Irma Lerma Rangel College of Pharmacy College Station campus, “but, on the other hand, why would companies spend in excess of two billion dollars and wait 10 or more years to develop a drug if they can’t make a huge profit? That’s the balance we need to strike.”
Adding to the risk is the possibility that drugs might be pulled from the market before they can make any money at all, and as many as 80 percent of the drugs that are sold don’t recover the amount of money spent on their development completely, according to Khan. At the same time, some blockbuster drugs manage to make billions of dollars, and that helps encourage drug companies to continue to create new medications. “It’s an extremely high-risk, but highly profitable business,” he said.
Khan sees the approval of generics and competition in the market as being key to driving down costs. “We have a very good system in place in the United States to allow generic drugs after a certain number of years of exclusivity,” said Khan, who was director of the Division of Product Quality Research at the Food and Drug Administration (FDA) before joining Texas A&M. “About 88 percent of prescriptions are generic, and those manufacturers are able to copy the formulas of the original drug and avoid the extensive safety and efficacy clinical trials in patient populations, which means the medication becomes very inexpensive.”
However, that’s only if the system works properly, and it doesn’t always. “Some brand products have been around a long time—and their exclusivity has long since expired—but there are still no generics,” Khan said. “That’s something the FDA needs to deal with more effectively.”
One reason for the lack of generics is that sometimes a brand name drug company will file a citizen petition with the FDA, saying that manufacture of the drug is risky and complicated and that if generics are allowed, they may cause problems. “Generic approvals get delayed because of these petitions, and the FDA may ask the generic company to do additional testing or need extended multiple cycle of responses,” Khan said. These citizen petitions and response cycle times have the potential to delay timely access to generic medications.
Generally, generics don’t have to undergo a lot of clinical pharmacodynamics studies or animal safety testing; they simply must show that their product has pharmaceutical equivalence and bioequivalence with the original drug—which provide an indication that it is also therapeutically equivalent. However, when the drug is something that is not absorbed into the body in sufficient quantities to be detected in the blood, bioequivalence can be difficult to prove. This is generally the case for locally acting antibiotics and anti-inflammatory drugs in the gastrointestinal tract, products topically applied to the skin or ocular products because their concentrations are not significant enough in the blood to measure and quantitate. Regulations do exist to do bioequivalence by in vitro laboratory studies, but there are not many published and peer-reviewed studies to show and validate what those in vitro studies are.
Still, there are ways to approach the problem if the brand name drug company is insisting on further testing. “The regulations do provide a window, it’s just that a scientific determination needs to be made,” Khan said. “If the generic is made exactly the same as the brand, then you can test its stability and release in the different environments that exist in the human body, and if the release of the drug is the same or very similar as the brand, then we propose that it is very likely they will behave similarly in a human being.” A precedence of this approval by in vitro procedures without clinical bioequivalence studies is provided by the approval of locally acting vancomycin antibiotic capsules.
Additionally, many generic products are made outside the United States. Inspections of those facilities are difficult and more complicated than inspection of domestic facilities. “Foreign facility inspections need to be streamlined and should be on par with the frequency of domestic inspections,” Khan said. “If they are not streamlined to ensure a consistently good quality generic product quality, we may see more problems of drug shortages with unexpected post-market failures.”
Khan sees bringing the industry back to the United States as a required remedy, but says we need many more trained professionals. “Pharmaceutical and biotech industry might create 350,000 new jobs in the next ten years with regulatory reforms, according to Steven Ubl, the head of Pharmaceutical Research and Manufacturing Association, or PhRMA, but we don’t have anywhere near that number of people trained in the pharmaceutical sciences,” Khan said. “We have to be self-sufficient and shouldn’t depend on drugs manufactured elsewhere, and there is a tremendous opportunity here for education and training.”
To that end, approval for master’s and doctorate programs in the College of Pharmacy is in the works, and Khan hopes students can begin taking classes in the fall of 2018. Collaboration is also key. “We need to bring our Health Science Center, engineering, veterinary medicine, AgriLife, life sciences and other programs together and have incentives for a multidisciplinary approach,” he said. “If people work together, there is no doubt they can bring down the cost with more efficient manufacturing processes, novel products and a more streamlined regulatory process.”
“We cannot go on like this forever—some of these medications are just so expensive,” Khan added, “but if we avoid the greed displayed by some that have been identified in the media recently, and work together as a nation, there is no reason we cannot dramatically cut down on the price.”